
- Surgery Archives
- Gallery Item
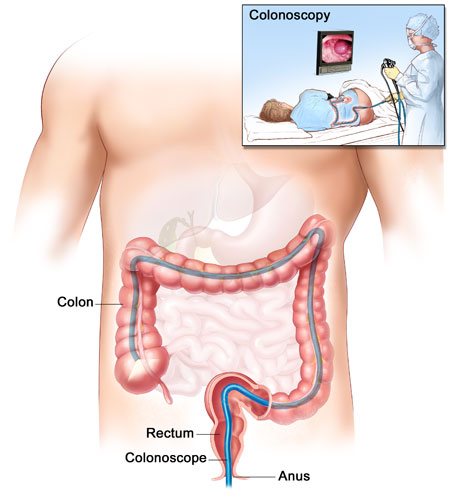
Colonoscopy
A whole lot of people avoid, put off, and just down right
refuse getting a colonoscopy. Especially if they don't have
any gastrointestinal issues, chronic belly pain, or change in
bowel habits. But let me tell you, better to "suffer" the
colonoscopy and know for sure and early than to wait and
find out late.
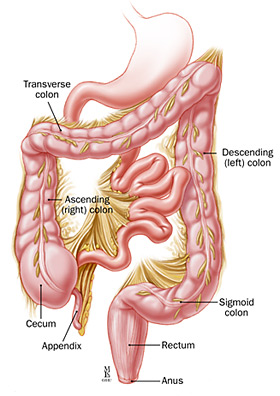
Colon Disorders
Anal fissures, abscesses, infections Oh My!. There can be a lot going on at that
end of the spectrum so it's best to take it slow and easy. A healthy diet and
cleanliness go along way here in reducing your risk.
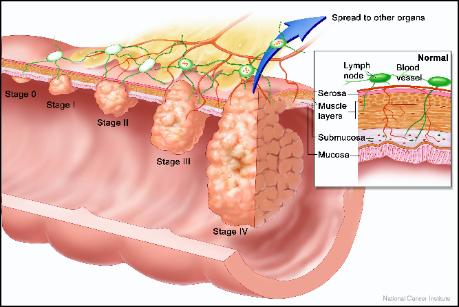
Colon Cancer
If you have cancer of the colon or rectum, your doctor will probably talk to you about
various treatment options. Surgery to remove the tumor is usually the main
treatment for colon and rectal cancer. Chemotherapy (treatment with drugs that kill
cancer cells) is often used when there is a risk that the colon or rectal cancer will
come back.
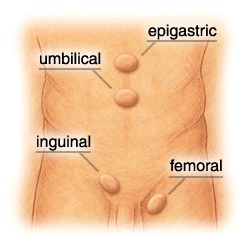
Hernia
A hernia is caused when the muscles of the abdomen develop a weak spot, or
defect, through which abdominal contents can bulge out. The contents of the hernia
are contained within a thin lining called the hernia sac.
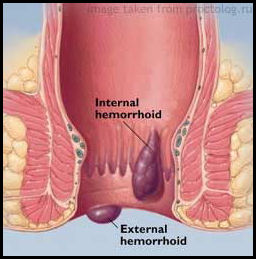
Hemorrhoids
External hemorrhoids are veins that lie just under the skin on the outside of the
anus. Sometimes, after straining, the external hemorrhoidal veins burst and a blood
clot forms under the skin. This is called a pile and is very painful.
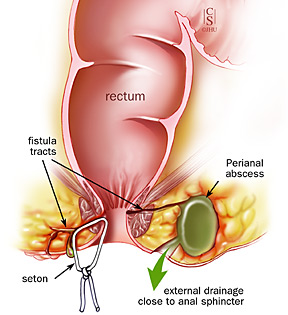
Perianal Abscess
When the tiny anal glands that open on the inside of the anus get blocked, the
bacteria that always live in the glands cause an infection. When pus forms, there is
an abscess (a pocket of pus). Treatment includes draining the abscess, usually
under local anesthesia in the doctor's office.
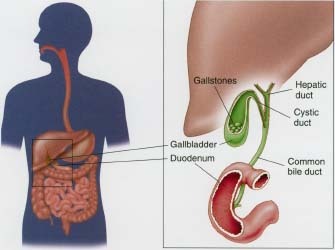
Gallbladder
The gallbladder is a small pear-shaped organ on the underside of the liver that is
used to store bile. Bile is made in the liver and is stored in the gallbladder until it is
needed to help the digestion of fat.
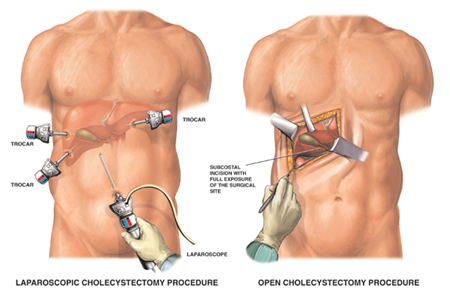
Gallbladder Surgery
A laparoscopic cholecystectomy is a surgical procedure in which your health care
provider removes your gallbladder with a laparoscope and other surgical tools. A
laparoscope is a thin metal tube with a light and tiny camera.
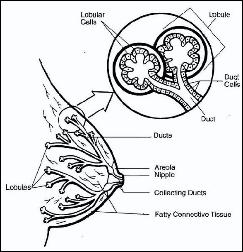
Breast Cancer
Breast surgery can be frightening because of the association with cancer. However,
80% of breast lumps are benign. Benign conditions such as breast abscess,
fibroadenomas, fibrocystic disease, breast pain and nipple discharge may require
surgery for diagnosis and treatment.